Three Steps Forward, Two Steps Back
The Continued Struggle to Treat Mental Illness in America
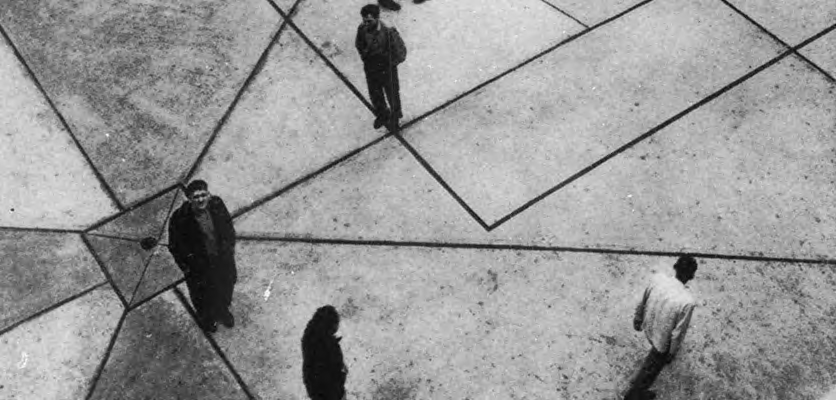
Picture a maze. The first steps in the path may start off clear and confident, but soon they hit a wall or false turn and must retreat and reevaluate. As with a maze, the response to mental illness throughout history has seen shifts and turns of imperfect progress.
This exhibit explores both societal and medical treatments of mental illness in the U.S. from the 18th century to today. It highlights institutional confinement, medical and pharmaceutical treatments, the development of child psychiatry, and the shift to police as mental illness first responders. Patterns of advancement and retreat carry through each case, showing the struggle to properly treat mental illness continues today.
Location: Eckenhoff Reading Room
Dates: Feb. 5 to July 31, 2026
Contact: ghsl-special
This exhibit was created to complement the National Library of Medicine’s traveling exhibit, Care & Custody: Past Responses to Mental Health, on display in the Galter Library atrium Feb. 9 - March 21, 2026.
Events
Galter Library hosted several events in conjunction with this exhibit and the NLM exhibit.
- Curator tour of the exhibit: Tuesday, Feb. 24, 12-1 p.m.; Thursday, March 19, 11 a.m.-12 p.m.; and Tuesday, April 14, 12-1 p.m.
- Special Collections Open House: Tuesday, March 3, 11 a.m. - 4 p.m. The Special Collections Reading Room is located on the second floor, at the top of the stairs (Room 2-411).
- Exhibit of memoirs written by people hospitalized for mental illness in Dollie’s Corner, available to check out. Curated by Lindsey O’Brien.
- Art activities in our craft corner in February 2026
The Rise of Institutionalization & Moral Treatment
At the turn the 18th century, ideas about mental illness were changing. Previously, people with mental illness had been tolerated at the margins of their communities, but never fully separated from them. Now, they were seen in conflict with the reason and rationality that Enlightenment thinkers believed would improve society. “Madness” became a threat to an ordered and civilized world. People with mental illness were incarcerated in so-called "lunatic asylums," where they could be gathered up and excluded from society. By confining people in these specialized institutions, physicians saw an opportunity to systematically observe and categorize their conditions, laying the foundations for the field of psychology.

This engraving, by satirist William Hogarth, is part a series of prints chronicling the downfall of an extravagant young man whose life of excess leads to poverty and eventually madness. It depicts the interior of Bethlehem Hospital, better known as “Bedlam,” and highlights the chaotic environment and neglect of the so-called “inmates” housed there, as well as the public perception of them. Fashionable women visit the asylum, watching the antics of the residents for their amusement. The figure in the foreground, with his shackled ankle, demonstrates the common use of chains to restrain inmates in asylums. By the turn of the 19th century, some reformers advocated for the removal of physical restraints, leading to more humane treatment.
In 1792, Quaker philanthropist William Tuke founded the Retreat, outside of York, England. Here, he and his family pioneered “moral treatment,” an approach to mental health care in direct opposition to the harsh treatment of earlier asylums.
Moral treatment (based on “morale,” not morality) appealed to the self-esteem and emotional wellbeing of patients, providing a comfortable and pleasant environment for them to recover. This relied on the proprietors’ belief that most mental illness was behavioral and curable; if patients could learn self-restraint and engage in productive activities, they could eventually be reintegrated into society.
Tuke’s grandson Samuel described the operation and philosophy of the Retreat in this 1813 book. Sections reflective of their innovative ideas include “Of the means of assisting the patient to control himself” and “Of the means of promoting the general comfort of the insane.”
...whatever tends to promote the happiness of the patient, is found to increase his desire to restrain himself... The comfort of the patients is therefore considered of the highest importance, in a curative point of view.
Moral Treatment Through Design
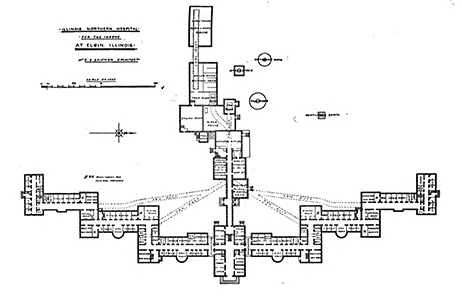
Inspired by the moral treatment movement, American physician Thomas Kirkbride attempted to standardize the buildings that held psychiatric patients, creating a pleasant but structured environment. His suggestions included separating patients into different wings by sex and by the severity of their illness, providing plenty of light and ventilation, and placing the building in a secluded pastoral setting with space for recreation as well as opportunities for productive employment.
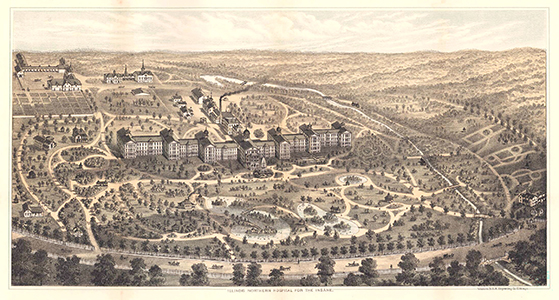
These so-called Kirkbride buildings sprung up across America starting in the 1840s. The Northern Illinois Hospital for the Insane (now the Elgin Mental Health Center) opened in 1872 with a Kirkbride-style building, seen in the floor plan below. The engraving below shows the grounds of the hospital c. 1885, including paths for strolling and farmland (upper left) that was tended by patients, providing the useful occupation seen as crucial to their recovery.
The Rise of Psychology
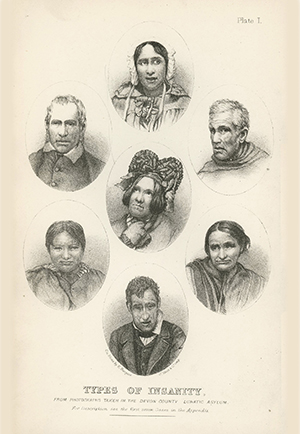
Before the underlying causes of mental illnesses were fully understood, one way of classifying them was by their symptoms and the physical appearance and behavior of patients, as illustrated in the frontispiece of this book. These representations of the “types of insanity” (including “acute mania” and “primary dementia”) would help doctors recognize and distinguish the conditions they might encounter in their work, often carried out in the secluded environment advocated by the Tuke family and Thomas Kirkbride.
This book was co-written by Daniel Hack Tuke, great-grandson of Retreat founder William Tuke. The authors review the work of the Retreat favorably alongside a more scientific discussion of the diagnosis and pathology of insanity. Their book was the standard English work on psychology for many years.
The moral treatment of insanity... consists [of] opposing the pre-occupation of delusion [with] ideas which are generated during useful occupation and wholesome recreation.
Shifting Narratives on Child & Adolescent Mental Illness
Pediatrics as a unique discipline and practice had only just emerged in the early 1800s, so it is unsurprising that the exploration into mental illness in children only began toward the end of that century. The first half of the 20th century saw a shift in theory and practice as the fields of child psychology and psychiatry developed. This case explores the growth of the study and perception of mental illness in children.
Moral Defects & Custodial Care, 1850 – 1900
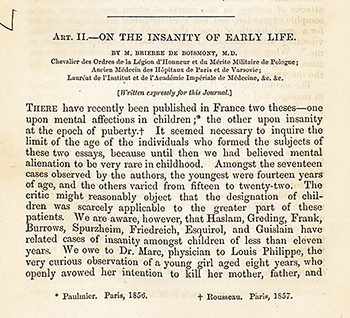
Until the mid-to-late 1800s, the idea of studying the young mind as a separate entity from the adult was non-existent. One of the earliest papers to discuss children and adolescent psychology was A. Brierre de Boismont’s "On the Insanity of Early Life" (1857), which held up the concept of behavioral or psychological challenges in youth as a “moral defect.” As with adults of the time, the response to these challenges was typically not diagnostic in nature, but rather focused on containment, either by parents and teachers, or alongside adults in “lunatic asylums.” These institutions were not meant to treat the children in their custody, but rather to separate them from society.
Delinquency & Child Guidance Movement, approx. 1900 – 1930
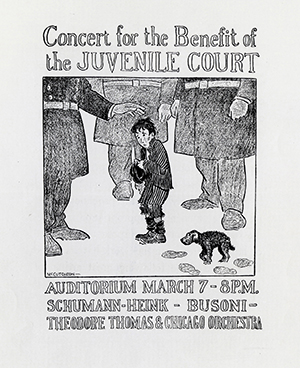
The Cook County Juvenile Court, established in 1899, is often discussed as a turning point in the recognition of psychiatric conditions in children and adolescents. Pioneers in this movement marked a shift from moralism to the idea of “maladjustment.” The women of Jane Addam’s Hull House, a charity founded in 1889 to serve the most vulnerable of society, were major players in the push to develop a juvenile justice system. They did not simply want a response to delinquency, however, and they later established the Chicago Juvenile Psychopathic Institute in 1909, which focused on uncovering the causes of delinquency in children.

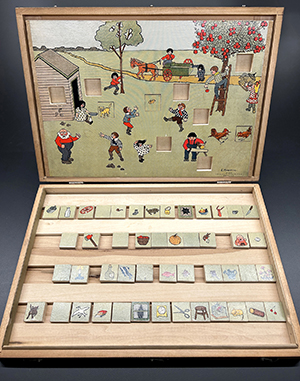
William Healy, MD, was hired as the first director of the Chicago Juvenile Psychopathic Institute. Throughout his career, Healy, in partnership with Grace Maxwell Fernald, developed several psychological tests including the Pictorial Completion Test (right), used into the 1920s. This test measured children’s apperception—how people make sense of new ideas according to what they already know—in this case, filling in the 10 blank squares with the most logical images based on visual cues in the picture. This test was meant to be used in conjunction with many other tests to determine a child’s "mental capacity," which could be a factor in delinquency. Each blank had one correct answer, and errors were tallied as logical or illogical. Scores with more than one illogical error or more than two total errors “should arouse suspicion of defect in mental ability.”
The performance gives a remarkably good chance to see the mind at work. Mental control and association processes are peculiarly laid bare, and for the study of these in defectives and aberrational individuals this type of test offers much.
Diagnostic Criteria & Treatment, approx. 1940 – 1950s
In 1937, Leo Kanner, MD, published Child Psychiatry, which is recognized as one of the first books on the subject. Kanner looked at individual personality disorders and sought to understand the range of potential causes, rather than focusing on a single explanation (environment, intelligence, heredity, etc.), as was common of the time.
In the following years, subspecialities and child-focused research would continue to develop. When the Diagnostic Statistical Manualwas published in 1952, children were briefly mentioned, but childhood-adolescence behavior disorders were not discussed separately until 1968’s DSM II.
On the Shift to the Child Guidance Movement
Children’s behavior problems came to be considered worthy of psychiatric attention for their own sake, because they existed and called for adequate guidance and not solely because of what might happen later in life.
On the Need for Thorough & Unbiased Diagnoses
Insistence on any ‘one and only’ cause, however, fails to do Justice to the wide variety of factors that may, and really do, combine themselves to produce the multitude of personality disorders which we find in different children.
Treatments In & Out of Hospitals
As knowledge of the human body expanded during the 18th and 19th centuries, new theories about the nature of the mind led to new treatments. In centuries past, people often blamed spiritual ill health for strange behaviors or thought patterns. Doctors and public health officials now turned to the central nervous system as the regulator of personality, thought and behavior.
While asylums and physical restraints largely aimed to separate those deemed incapable of “normal” functioning from the rest of society, both science and pseudoscience attempted to recalibrate nervous system functions. A range of treatments attempted to “rewire” or even “shock” the brain into working differently.
Electrotherapy

As early as the 1700s scientists explored using electricity in medicine. While early experiments paved the way for everything from the Automated External Defibrillator (AED) to transcranial magnetic stimulation (TMS), they also inspired money-grabs and the painful electroconvulsive therapy treatments made infamous in films such as One Flew Over the Cuckoo’s Nest. Davis and Kidder’s machine, displayed here, was patented in 1854 and followed the common quack narrative of promising to cure everything from hiccups to epilepsy.
Published in 1887, Electricity as Medicine serves as a manual for similar electrical devices and features an entire chapter titled “Disorders of the Brain and Spinal Cord,” which begins, “As the brain is conceded to be the seat of the mind, so we conclude that disturbances of the understanding are the natural results of derangement of that organ." The following pages detail how electricity treats “hypochondria,” “cerebral exhaustion,” both brain “congestion” and “anaemia,” catalepsy, “ecstasy," “congestion of the spine" and “spinal irritation."
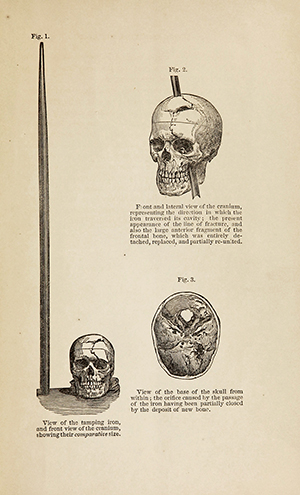
In 1848, Phineas Gage was working as a railroad construction foreman when an explosion drove a 3’ 7” long tamping iron through his face and head, destroying eyesight in his left eye, and much of his left frontal lobe. Though he survived, in subsequent years, friends of Gage reported drastic changes in his personality, leaving him more volatile and sometimes violent. John M. Harlow, MD, detailed the injuries and behavioral changes in the above 1869 pamphlet. Incidences such as this clearly pointed toward the importance of the brain itself in controlling human behavior.
Psychosurgery
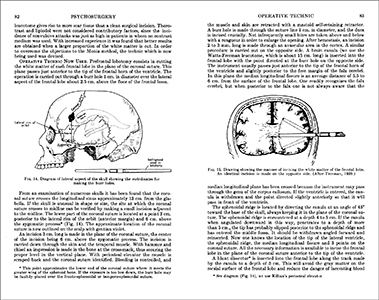
Lobotomy, though not a direct descendant of Gage’s accident, also severed the frontal lobe, resulting in personality changes. Walter Freeman and James W. Watts popularized lobotomy in the U.S. in the 1930s and ‘40s. Watts later broke with Freeman when he introduced the transorbital method of lobotomy. Colloquially known as the “icepick” method, it was performed with a long, pointed tool resembling a household icepick inserted through a patient’s eye socket. Freeman insisted it could be performed safely by non-surgeons as an outpatient procedure. Subsequently, approximately 40,000 people were lobotomized in the United States through the 1970s. Aside from emotional blunting, common side effects of the procedure include incontinence, epilepsy and loss of cognitive function. Freeman called post-lobotomy life “surgically induced childhood,” more than hinting at common paternalistic attitudes toward mental health patients.
Psychopharmacology
The late 19th to mid 20th century saw the development of a range of pharmaceuticals, such as alkaloids, barbiturates and benzodiazepines, for mental health conditions. Research and production booms drove the development of new pharmaceuticals between and after the two world wars.
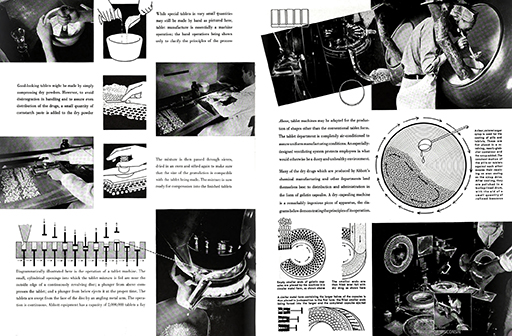
Abbott Laboratories was founded in Chicago in 1888. This promotional booklet from 1938 boasts about the pharmaceutical company’s production-scale, state-of-the art research facilities and sleek equipment.
Metrazol (pentylenetetrazol)
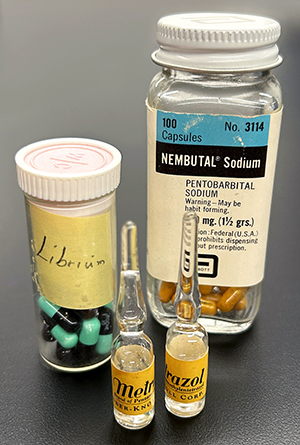
Beginning in the 1930s, this stimulant was used in convulsive therapy, which was replaced by electroconvulsive therapy for the treatment of depression. Metrazol’s FDA approval was revoked in 1982.
Metrazol. Bilhuber Knoll Corp. Orange, NJ, approximately 1940. 2018.05.006.
Librium (chlordiazepoxide)
The original benzodiazepine, this medication was patented in 1958 and prescribed for sedative and anxiolytic effects. Today benzodiazepines such as Xanax and Ativan have widely replaced the early barbiturate class of medication.
Librium. Hoffmann-Roche. Basel, Switzerland, approximately 1960. 2018.05.006.
Nembutal (pentobarbital)
First introduced in the 1930s, this short-acting barbiturate is typically used as a sedative, an emergency anti-convulsant and as a pre-anesthetic. Barbiturates were sometimes prescribed for anxiety or insomnia. Risk of physical dependence or overdose on barbiturates became increasingly recognized in the early 1960s.
Nembutal. Abbott Laboratories. North Chicago, IL, approximately 1950. 2018.05.006.
Chicago’s Approach to Mental Illness: From Institution to Community
In 1963, President Kennedy signed the Community Mental Health Act (CMHA) into law. It sought to decrease the patient population in state-run psychiatric hospitals by shifting care to publicly funded community mental health centers (CMHCs). Congress would provide construction and initial operating funds, then state and local governments were expected to take over.
Decreasing the psychiatric inpatient population by 50 percent was achieved in 1977, but CMHCs lagged far behind. It was estimated that 2,000 centers were needed to provide nationwide coverage for essential mental health services. By 1975, just 650 centers had opened, nowhere near the amount needed to treat those who had already been discharged from psychiatric hospitals.
As both hospital beds and CMHCs disappeared, people with mental illness were left with few options. According to the Chicago Policy Review, this "has resulted in overreliance on the police to respond to both mental health crises and everyday interactions with people with mental illnesses."
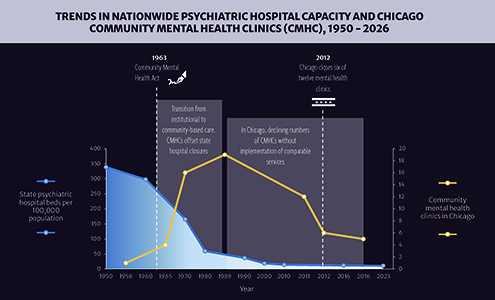
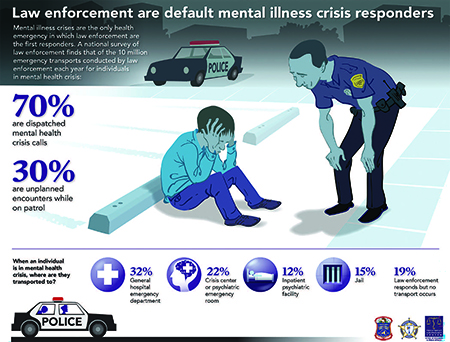
The visualization above illustrates the decline in psychiatric hospital capacity in the U.S. and the concurrent fluctuation in community mental health clinics in Chicago over the last 75 years. CMHCs reached their peak in Chicago in the 1970s to '80s, but once funds were no longer earmarked for mental healthcare, they were vulnerable to spending cuts and closure. These closures coupled with a shortage of psychiatric inpatient beds have left people with nowhere else to go. The infographic and quotes below show how police have been forced to fill the void, often without crisis intervention training.
The Community-Based Model
The community-based model for the treatment of mental illness gained traction in American psychiatry in the postwar era. It argued that psychiatric hospitals subjected many people living with mental illness to inappropriate or harmful treatments and kept them isolated. Moving care into the community would allow people to integrate with society during and after treatment.
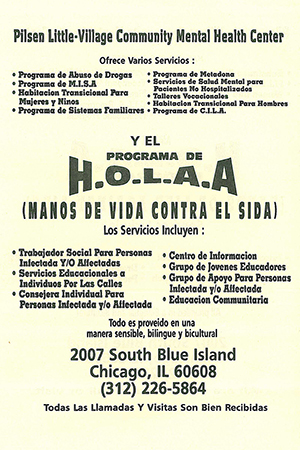
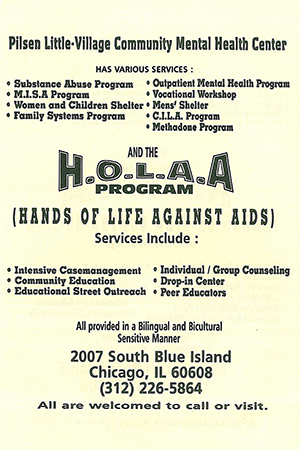
Beyond the relocation of treatment, the CMHA encouraged local communities to tailor mental health services to their needs and to organize the centers according to the area’s demographics. This flyer advertising the Pilsen Little-Village Community Mental Health Center highlights services relevant to the immigrant-rich neighborhood and the center’s commitment to cultural competency.
Optimism Without Infrastructure
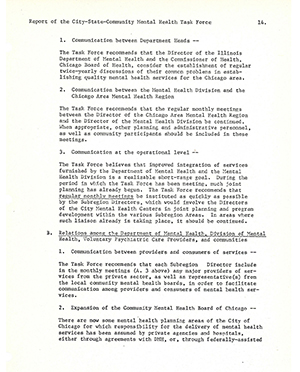
In January of 1971, the directors of the Chicago Board of Health and the Illinois Department of Health commissioned a task force to study the uneven distribution of mental health services across Chicago and to make recommendations for specific neighborhoods as well as the entire system.
The top three recommendations of this report—communication, relationships and collaboration—show, in microcosm, why the CMHA failed to achieve its goal of comprehensive mental healthcare at the community level: too little structure. The CMHA did not mandate any overarching infrastructure to integrate the new CMHCs into the preexisting mental health system.
Without oversight or an administrative framework, communication channels between state hospitals and CMHCs failed, relationships festered, long-term planning was not coordinated and there was a lack of accountability. This all led to disparate standards of care between communities as well as an unstable and ineffectual national system.
Police as Street-Corner Psychiatrists
Research using data from 2008-2016 found that these closures did not increase arrest rates, but they did lead to more police contact and police-initiated mental‑health transports to hospitals. With fewer community resources available, people in crisis often end up calling 911, shifting responsibility for mental health response onto law enforcement.
As of March 2025, about 26 percent of Chicago’s sworn officers had completed Crisis Intervention Team (CIT) training and only 45 percent of nearly 55,000 mental‑health‑related calls in 2024 were handled by a CIT‑trained officer. Regardless of their training, officers are frequently placed in the role of “street‑corner psychiatrists,” tasked with assessing whether an individual is experiencing a mental health crisis, and if so, determining next steps. In the absence of adequate community resources, the options available to officers in these moments are limited, often insufficient for supporting the long‑term well‑being of people living with mental illness.
Recent Studies in Chicago
High rates of behavioral health calls are observed in areas with closed CMHCs.
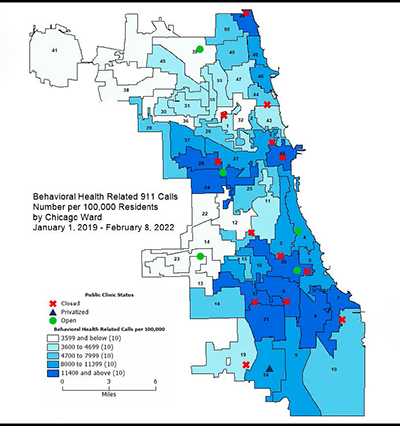
In the absence of accessible, affordable mental healthcare, “mental health needs often go unaddressed until they reach a point of crisis.” Individuals experiencing a mental health crisis, their loved ones or observers call 911 for assistance, and police are dispatched.
Personal Experiences of Police Encounters During Mental Health Crises
There’s shame and criminalization and acute embarrassment and mortification in being picked up by the police for being ill.
Bradbury et al. “Lived Experience of Involuntary Transport under Mental Health Legislation.” Int J Ment Health Nurs 26, no. 6 (Dec 2017): 580-92.
Once they [the police] took me to hospital, and left me there assuming I would see a...mental health care professional... But nobody did see me, they just unstrapped me and I went home.
When I was taken to hospital, the officer was kind and did not show signs of stigma.
I’ve got these guys on their radios and yelling down from the balcony of my seventh floor down to the other people, about my condition, to my neighbours all listening in. …I had a private medical crisis and they made it public.
I realized that they [the police] were trying to help me. But when they are putting handcuffs on ya, and dragging you around, you don’t think that way. …They were trying to prevent harm, harm to myself, and self-harm.
Brink et al. A Study of How People with Mental Illness Perceive and Interact with the Police. Mental Health Commission of Canada (Calgary, Alberta: 2011).
Perspectives From Chicago Police Officers
They [call subjects] always feel betrayed, like you brought ‘em to the hospital and they just gonna stick ‘em with needles, strap ‘em to the bed, and fill ‘em with medication, which usually happens, but can we do it in a different way, you know?
We take ‘em there [a hospital]. Once we release them to the mental facility don’t know what happens to ‘em. Obviously it’s not working because they’re right back on the street doing the same thing. So there’s a disconnect between the follow-through and the resources.
Watson and Wood. “Everyday Police Work during Mental Health Encounters: A Study of Call Resolutions in Chicago and Their Implications for Diversion.” Behav Sci Law 35, no. 5-6 (Sep 2017): 442-55.
Insight From a Chicago Expert
There’s a power imbalance there, especially when police are first responders…People might, technically, agree to go to the hospital because they’re met with no other option, but that agreement is happening in the presence of an armed officer, so under the threat of force without fully understanding their rights or true alternatives.
McGhee et al. “Shadow Arrests: Chicago Police Make Growing Use of Forced Psychiatric Hospitalization.” South Side Weekly (Chicago, IL), Aug 28, 2025: 18-23.
The Continued Struggle
Stories from people with mental illness and from law enforcement officers, in Chicago and beyond, highlight several themes:
Inconsistency: Individuals and their families experience a range of encounters with police, from supportive to traumatic. Officers themselves noted that responses to behavioral health calls depend on an officer’s training, comfort level and attitude toward mental illness.
Stigma and criminalization: Individuals in crisis often feel intense shame as the presence of police draws spectators. Practices such as handcuffing or transporting someone to the hospital in the back of a squad car can deepen feelings of embarrassment and reinforce stigma.
Limited follow-through: Regardless of the relatively positive or negative nature of the interaction, individuals receive little long-term support. Many officers consider hospital transport a reset, a method of getting an individual safely through the immediate crisis, but without long-term solutions to prevent future ones.
Credits
Curated by Emma Florio, MLIS, Archives & Research Specialist; Katie Lattal, MA, Special Collections Librarian; Corinne Miller, MLIS, Clinical Librarian; Lindsey O’Brien, MSLIS, Cataloging & Metadata Librarian; and Annie Wescott, MLIS, Research Librarian.
Designed by Katie Lattal and Emma Florio.
Bibliography
Moral Treatment
- Bockover, J. Sanbourne. Moral Treatment in American Psychiatry. New York: Springer Publishing Company, 1963. https://research.ebsco.com/linkprocessor/plink?id=e3108f00-7fb2-31d2-bb08-ed6c947c17f2
- Bucknill, J.C., and D.H. Tuke. A Manual of Psychological Medicine... 4th ed. London: J. & A. Churchill, 1879. https://catalog.hathitrust.org/Record/001587747
- Burdett, Henry C. Hospitals and Asylums of the World: Their Origin, History, Construction, Administration, Management, and Legislation. London: J. & A. Churchill, 1891. https://catalog.hathitrust.org/Record/001581280
- Grob, Gerald N. Mental Institutions in America: Social Policy to 1875. New York: Free Press, 1972.
- Grob, Gerald N. Mental Illness and American Society, 1875-1940. Princeton: Princeton University Press, 1983. https://www.fulcrum.org/concern/monographs/8623hz10x
- Hogarth, William. “Plate 8 (Tom Rakewell Ends up in the Bethlehem Hospital Madhouse)” from A Rake’s Progress. Etching and engraving. 1735. https://risdmuseum.org/art-design/collection/plate-8-tom-rakewell-ends-bethlehem-hospital-madhouse-522288
- Kirkbride, Thomas S. On the Construction, Organization and General Arrangements of Hospitals for the Insane. Philadelphia: Lindsay & Blakiston, 1854. https://catalog.hathitrust.org/Record/008595368
- Mehr, Joseph. An Illustrated History of Illinois Public Mental Health Services, 1847 to 2000. Victoria, B.C.: Trafford Publishing, 2002.
- Tinworth, Joanna. “A Rake’s Progress VIII: The Madhouse.” Sir John Soane’s Museum Collection Online. 2021. https://collections.soane.org/object-p47
- Tuke, Samuel. Description of the Retreat, an Institution near York, for Insane Persons of the Society of Friends... York: W. Alexander, 1813. https://wellcomecollection.org/works/dcy3yd8x
- Tuke, Samuel. Practical Hints on the Construction and Economy of Pauper Lunatic Asylums. York: William Alexander, 1815. https://archive.org/details/39002011122984.med.yale.edu/
- Western Bank Note & Engraving Co. “Illinois Northern Hospital for the Insane.” Engraving. Chicago. From Tucker, G.A. Lunacy in Many Lands... n.p., [1885?]. https://catalogue.nla.gov.au/catalog/2438921
Children and Adolescents
- Addams, Jane. “The Bad Boy of the Street.” Ladies’ Home Journal 26 (October 1909): 17, 76. https://babel.hathitrust.org/cgi/pt?id=mdp.39015011414250&seq=322
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2nd ed. Washington, DC: American Psychiatric Association, 1968. https://www.madinamerica.com/wp-content/uploads/2015/08/DSM-II.pdf
- Brierre de Boismont, A. “On the Insanity of Early Life.” Journal of Psychological Medicine and Mental Pathology 10, no. 8 (1857): 622–638. https://pmc.ncbi.nlm.nih.gov/articles/PMC5091123/
- Department of Psychiatry. "History." University of Illinois Chicago. n.d. Accessed January 7, 2026. https://www.psych.uic.edu/about-us/history
- Gingell, Kate. “The Forgotten Children: Children Admitted to a County Asylum between 1854 and 1900.” Psychiatric Bulletin of the Royal College of Psychiatrists 25, no. 11 (2001): 432–434. https://doi.org/10.1192/pb.25.11.432
- Healy, William. “A Pictorial Completion Test.” Psychological Review 21, no. 3 (1914): 189–203. https://doi.org/10.1037/h0075712
- Hull-House Photograph Collection. University of Illinois Chicago. Accessed January 7, 2026. https://digital.library.uic.edu/view/ark:/81984/d3vd6pc7j
- "Illinois Supreme Court History: Juvenile Courts." Illinois Courts. June 23, 2020. https://www.illinoiscourts.gov/News/388/Illinois-Supreme-Court-History-Juvenile-Courts/news-detail/
- Jane Addams Hull-House Association. "Jane Addams and Child Protection." n.d. Accessed December 3, 2025. https://janeaddamshullhouse.org/history/jane-addams-and-child-protection/
- Kanner, Leo. “The Psychopathological Problems of Childhood.” In Practical Clinical Psychiatry, 5th ed., edited by Edward A. Strecker, Franklin G. Ebaugh, and Leo Kanner. Philadelphia: The Blakiston Company, 1940. https://catalog.hathitrust.org/Record/002066736
- Rhoades, M. Carter. A Case Study of Delinquent Boys in the Juvenile Court of Chicago. Chicago: The University of Chicago Press, 1907. https://catalog.hathitrust.org/Record/001135857
Medical Treatments
- Abbott Laboratories. Abbott, Servant to Medicine. Chicago: Runkle-Thompson-Kovats, 1938. https://catalog.hathitrust.org/Record/001575765
- Ban, Thomas A. “Fifty years chlorpromazine: a historical perspective.” Neuropsychiatr Dis Treat 3, no. 4 (August 2007): 495-500. https://pmc.ncbi.nlm.nih.gov/articles/PMC2655089/
- Benzodiazepine Information Coalition. “A Brief History Of Benzodiazepines.” n.d. https://www.benzoinfo.com/a-brief-history-of-benzodiazepines/
- Freeman, Walter and James W. Watts. Prefrontal lobotomy in the treatment of mental disorders. Psychological Cinema Register, Pennsylvania State College, 1942. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-8800490A-vid
- Freeman, Walter and James W. Watts. Psychosurgery: Intelligence, Emotion and Social Behavior following Prefrontal Lobotomy for Mental Disorders. Springfield, Ill.: Charles C. Thomas, 1942. https://catalog.hathitrust.org/Record/102194621
- Harlow, J.M. Recovery from the Passage of an Iron Bar through the Head. Boston: David Clapp & Son, 1869. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-66210360R-bk
- Hillhouse, Todd M., and Joseph H. Porter. “A brief history of the development of antidepressant drugs: From monoamines to glutamate.” Exp Clin Psychopharmacol 23, no. 1 (February 2015): 1-21. https://pmc.ncbi.nlm.nih.gov/articles/PMC4428540/
- PharmaPhorum. “A history of the pharmaceutical industry.” September 1, 2020. https://pharmaphorum.com/r-d/a_history_of_the_pharmaceutical_industry
- Holland, Ryan, David Kopel, Peter W. Carmel, and Charles J. Prestigiacomo. “Topectomy versus leukotomy: J. Lawrence Pool’s contribution to psychosurgery.” Neurosurgical Focus 43, no. 3 (2017): E7. https://doi.org/10.3171/2017.6.FOCUS17259
- Ives, John. Electricity as a Medicine and Its Mode of Application. New York: Galvano-Faradic Mfg. Co., 1887. https://catalog.hathitrust.org/Record/100165997
- Journal of the American Pharmaceutical Association 1, no. 8 (1961): 491
- López-Muñoz, Francisco, Ronaldo Ucha-Udabe, and Cecilio Alamo. “The history of barbiturates a century after their clinical introduction.” Neuropsychiatr Dis Treat 1, no 4 (December 2005): 329-343. https://pmc.ncbi.nlm.nih.gov/articles/PMC2424120/
- Neurology 6, no. 11 (1956): 754.
- Orkaby, Asher and Sukumar P. Desai. “The Death of Sodium Pentothal: The Rise and Fall of an Anesthetic Turned Lethal.” J Hist Med Allied Sci 76, no. 3 (July 2021): 294-318. https://doi.org/10.1093/jhmas/jrab016
- Pow, Joni Lee, Alan A. Baumeister, Mike F. Hawkins, Alex S. Cohen, and James C. Garand. “Deinstitutionalization of American Public Hospitals for the Mentally Ill Before and After the Introduction of Antipsychotic Medications.” Harvard Review of Psychiatry 23, no. 3 (May/June 2015): 176-187. https://www.lsu.edu/hss/psychology/faculty/biological/SecondHarvardReviewPaper.pdf
- Rogers, Kara. "Insulin shock therapy". Encyclopedia Britannica. May 26, 2023. https://www.britannica.com/science/insulin-shock-therapy
- Wood Library Museum of Anesthesiology. “Magneto-Electric Machine.” Museum Collection, Alternative Medicine. https://www.woodlibrarymuseum.org/museum/magneto-electric-machine/
Chicago's Approach
- Adams, Dani. "Democratizing Mental Health." South Side Weekly (Chicago), February 4, 2020. https://southsideweekly.com/mental-health-advocates-put-public-services-back-on-table/
- Bradbury, J., M. Hutchinson, J. Hurley, and H. Stasa. "Lived Experience of Involuntary Transport under Mental Health Legislation." Int J Ment Health Nurs 26, no. 6 (Dec 2017): 580-92. https://doi.org/10.1111/inm.12284
- Bradford, Shannon. "The History of Community Mental Health Care." The Chicago Policy Review (March 12, 2021). Accessed December 12, 2025. https://chicagopolicyreview.org/2021/03/12/community-mental-health-care-lessons-from-history/
- Brink, J., J. Livingston, S. Desmarais, C. Greaves, V. Maxwell, E. Michalak, R. Parent, S. Verdun-Jones, and C. Weaver. A Study of How People with Mental Illness Perceive and Interact with the Police. Mental Health Commission of Canada (Calgary, Alberta: 2011). https://mentalhealthcommission.ca/research/research/a-study-of-how-people-with-mental-illness-perceive-and-interact-with-the-police/
- Burke, Nancy, and Angela Sedeño. "The Kedzie Center: Community-Immersed Health from the Ground Up." Int J Appl Psychoanal Studies 20 (May 2023): 178-89. https://doi.org/10.1002/aps.1816
- City-State-Community Mental Health Task Force. City-State-Community Mental Health Task Force Report. [Chicago]: City-State-Community Mental Health Task Force, 1972.
- Collaborative for Community Wellness. 911 Behavioral Health Call Rates Across Chicago’s Wards: Understanding Call Rates in the Context of Disinvestment in Public Mental Health Services. January 1, 2022. https://collaborativeforcommunitywellness.org/911-behavioral-health-call-rates-across-chicagos-wards-understanding-call-rates-in-the-context-of-disinvestment-in-public-mental-health-services/
- Erickson, Blake. "Deinstitutionalization through Optimism: The Community Mental Health Act of 1963." American Journal of Psychiatry Residents’ Journal 16, no. 4. (June 2021): 6-7. Accessed January 5, 2026. https://doi.org/10.1176/appi.ajp-rj.2021.160404
- Harcourt, Bernard E. "Reducing Mass Incarceration: Lessons from the Deinstitutionalization of Mental Hospitals in the 1960s." Ohio State Journal of Criminal Law 9, no. 1. (2011): 53-88. Accessed January 5, 2026. https://heinonline.org/HOL/P?h=hein.journals/osjcl9&i=55
- Lydersen, Kari. "‘Falling through the Cracks’." The Chicago Reporter, April 27, 2015. https://www.chicagoreporter.com/falling-through-the-cracks/
- McGhee, J., D. Brozost-Kelleher, I. Senechal, S. Stecklow, J. Mayzouni, A. Miglietta, and S. Ocneanu. "Shadow Arrests: Chicago Police Make Growing Use of Forced Psychiatric Hospitalization." South Side Weekly (Chicago), August 28, 2025. https://southsideweekly.com/shadow-arrests-chicago-police-make-growing-use-of-forced-psychiatric-hospitalization/
- Morrissey, Joseph P., and Howard H. Goldman. "Care and Treatment of the Mentally Ill in the United States: Historical Developments and Reforms." The Annals of the American Academy of Political and Social Science 484 (March 1986): 12-27. https://www.jstor.org/stable/1045181
- Musto, David F. "Whatever Happened to 'Community Mental Health?'" The Public Interest 39 (Spring 1975): 53-79. https://www.nationalaffairs.com/public_interest/detail/whatever-happened-to-community-mental-health
- Pilsen Little-Village Community Mental Health Center [flyer]. Tracy Baim Editorial Files, Windy City Box N (Alexander Street Press). LGBT Thought and Culture Database. Accessed 7 Jan. 2026.
- Sharfstein, Steven S. "Whatever Happened to Community Mental Health?" Psychiatric Services 51, no. 5. (May 2000): 616-20. Accessed January 6, 2026. https://doi.org/10.1176/appi.ps.51.5.616
- Smith, Michelle R. "50 Years Later, Kennedy’s Vision for Mental Health Not Realized." The Seattle Times, October 20, 2013. https://www.seattletimes.com/nation-world/50-years-later-kennedyrsquos-vision-for-mental-health-not-realized/
- Torrey, E. Fuller. Nowhere to Go: The Tragic Odyssey of the Homeless Mentally Ill. 2 ed. Springer Cham, 2025. https://doi.org/https://doi.org/10.1007/978-3-031-84685-4
- Treatment Advocacy Center. Road Runners: The Role and Impact of Law Enforcement in Transporting Individuals with Severe Mental Illness, a National Survey. May 2019. https://www.tac.org/reports_publications/road-runners-the-role-and-impact-of-law-enforcement-in-transporting-individuals-with-severe-mental-illness/
- Watson, A. C., and J. D. Wood. "Everyday Police Work during Mental Health Encounters: A Study of Call Resolutions in Chicago and Their Implications for Diversion." Behav Sci Law 35, no. 5-6 (Sep 2017): 442-55. https://doi.org/10.1002/bsl.2324